
What is pharmacodynamics?
The pharmacodynamics term derived from two words, pharmacon means a drug, and dynamics means action or activity of the drugs.
The simple meaning of pharmacodynamics is “ what the drug does to the body”. It deals with the study of the biochemical and physiological effects (activity) of drugs and their mechanisms of action (MOA).
Where the two drugs may show the same effects but their site of action may differ for example pilocarpine and morphine have almost the same effects but their site of action is different.
Types of drugs action: (“pharmacodynamics”)
It is the initial combination of the drug with its receptor resulting in conformational changes in the latter (agonists), or prevention of conformational changes through the exclusion of the agonist (means antagonist). There are the following types of drug actions including;
- Stimulation
- Depression
- Irritation
- Replacement
- Cytotoxic action
Stimulation
Some drugs stimulate and increase the activity of some specific organs or systems. For example; adrenaline drugs stimulate the heart resulting in an increase in heart rate and force of contraction in the body.
Depression
Some drugs depress or decrease the activity of some specific organs or systems in the body. For example, alcohol, barbiturates, general anesthetic drugs, etc. depress the central nervous system (CNS) in the body.
Irritation
When some drugs are used in topical routes they show irritation in the specific area when you can use drugs. Generally, irritation occurs when topical uses on the skin and adjacent tissues.
The skin relieves deep-seated pain which is called counterirritant, for example, eucalyptus oil, methyl salicylate, etc. These irrational drugs are useful in sprains, joint pain, and myalgia.
They exert their action by the following mechanism such as;
- Reflexly increasing local circulation in deeper structures in the body
- By the method of blocking impulse conduction in the spinal cord in the body.
Replacement
When a body has a deficiency of an endogenous substance it can be replaced by using a drug. For example, insulin used for diabetes mellitus, where is thyroxine used in cretinism and myxedema, etc.
Cytotoxic action
When some selective drugs are toxic for the infecting organism or cancer cells. For example, antibiotics or anticancer drugs.
Drugs effect
It is the ultimate change in biological function in the body brought about as a consequence of drug action, through a series of intermediate steps in the body.

Mechanism of drug action: (“pharmacodynamics”)
The mechanism of drug action is two types on the basis of a receptor, they are receptor-mediated and non-receptor-mediated.
Non-receptor mediated MOA
There are various types of the mechanism of drug action including;
- By physical action: osmosis, adsorption, demulcent, and radioactivity
- By chemical action:
- a combination of chemical compounds, for example, antacids are weaker bases they neutralize gastric acid and useful for peptic ulcer, etc.
- Through the enzymes:
- drugs act by inhibiting the activity of enzymes. They are enzyme inhibition or induction.
- Through the ion channels:
- Drugs are directly bound with ion channels and alter the flow of ions in the action area, for example, local anesthetics drugs block sodium ion channels in the neuronal membrane to produce local anesthetic action.
- Through antibody production:
- Some vaccines produce their effect by stimulating the formation of antibodies in the body, for example, a vaccine against tuberculosis (BCG), etc.
- Through transporter
- Many drugs produce their pharmacological action by directly interacting with the solute carrier class of transporter proteins,
- for example, fluoxetine inhibits neuronal reuptake of 5-HT by interacting with serotonin receptors in the body, etc.
Receptor-mediated mechanism: (“pharmacodynamics”)
What are receptors?
Receptors are macromolecule or binding sites located on the surface, cytoplasm, or inside the effector cell (nucleus) that serves to recognize the signal molecule or drug and initiate the response to it, but itself has no other function.
The receptor molecules are the ligand-binding domain and effector domain which undergo functional conformation changes. Drugs bind to the receptor and form a drug-receptor complex and response occurred.
- Affinity: The ability to bind with the receptor
- Intrinsic activity: The capacity to induce a functional change in the receptor
Agonist
Some drugs bind to physiological receptors and mimic the regulatory effects of the endogenous signaling compounds. Agonists have a high affinity as well as high intrinsic activity (e.g. morphine and adrenaline).
Antagonist
Some drugs that block or reduce the activity of an agonist but no stimulatory action of their own still may produce useful effects.
The competitive antagonist has a high affinity but without any intrinsic activity, for example, Naloxone and atropine produce receptor blockade.
Inverse agonists
Inverse agonists have a complete affinity for the receptor, but the effect is opposite to that of agonists.
For example, benzodiazepines produce anti-anxiety and anti-convulsant effects in the following ways by interacting with benzodiazepine (BDZR) receptors, but β-carbolines that act as an inverse agonist at benzodiazepine receptors and produce anxiety and convulsions.
It has affinity but intrinsic activity between 0 to -1 (example, β-carbolines).
Partial agonists
The drug binds to the receptor but produces an effect less than that of an agonist in the body. They inhibit the effect of agonist drugs. It has affinity but less intrinsic activity (e.g. buprenorphine and pindolol).
What is a ligand?: (“pharmacodynamics”)
Ligand is derived from Latin: ligare means to bind and it is defined as any molecule which attaches selectively to particular receptors or sites.
The term ligand only refers to affinity or binding capacity, regardless of functional changes: both agonist and antagonist (competitive) are ligands for the same receptor.
Receptor families: (“pharmacodynamics”)
They are following four types of general receptor including
- Ligand-gated ion channel (ionotropic receptors)
- G-protein-coupled receptors (metabotropic receptors)
- Enzyme receptors
- Receptor regulating gene expression
Ligand-gated ion channel receptor
It is also called ionotropic receptors which have 232 distinct-ion channels. Their onset of action drugs is fastest.
These cell surface receptors (ligand-gated ion channels) enclose selective ion channels for Na+, Ca+2, K+, or Cl-, etc within their molecules.
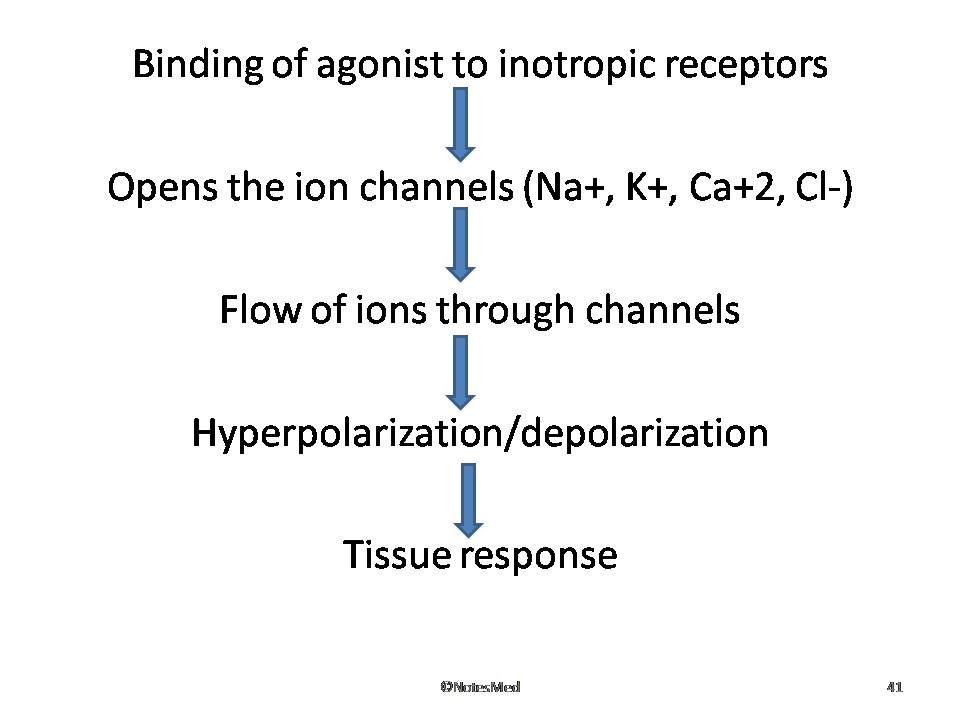
Agonist binding opens the channels and causes depolarizing or hyperpolarizing or changes in cytosolic ionic composition, depending on the ion that flows through it. For example, nicotinic cholinergic, GABA-A, glycine, 5-HT3 receptors fall in this category.
G-protein-coupled receptors (GPCR)
It is also called metabotropic receptors and over 800 GPCRs. These are large families of cell membrane receptors that are linked to the effectors (such as enzyme or channel or carrier protein) through one or more GTP-activated proteins (G-proteins) for response effectuation.
The molecule has 7α -helical membrane-spanning hydrophobic amino acid segments which run into 3 extracellular and 3 intracellular loops.

The agonist binding site is located somewhere around the helices on the extracellular face. There are 3 major effectors pathways through which GPCRs function:
- Adenylyl cyclase: cAMP pathway
- Phospholipase C: IP3-DAG pathway
- Opening or closing of ionic channels through activated G-proteins
Enzyme-linked receptors
This is a receptor that has a subunit with enzymatic properties or binds a JAK (Janus Kinase) enzyme activation.
The agonist binding site and the catalytic site lie respectively on the outer face and inner face of the plasma membrane in the site. There are two major subgroups of these receptors.

- Those having an intrinsic enzymatic activity (intrinsic enzyme receptors)
- Those that lack intrinsic enzymatic activity, but bind a JAK-STAT kinase on activation (JAK-STAT kinase binding receptors).
Receptor regulating gene expression
There are intracellular (nuclear or cytoplasmic) soluble proteins that respond to lipid-soluble chemical messengers that penetrate the cell
Dose-response curve: (“pharmacodynamics”)
The pharmacological effect of the drug depends on its concentration at the site of action, which in turn is determined by the dose of the drug you can administer.
Types of a dose-response curve
Graded dose-response
The graded dose-response curve is drawn on a graph in the form of a rectangular hyperbola with an S-shaped logarithmic dose-response curve.
Quantal dose-response curve
In certain pharmacological effects which cannot be quantified but can only be said to be present or absent (all or none) in the action, for example, a drug causing ovulation.
Potency
The graded dose-response curve is drawn on a graph in the form of a rectangular hyperbola with an S-shaped logarithmic dose-response curve.
Therefore, Morphine has ten times more potent than pethidine as an analgesic nature.
Efficacy
The maximal response that can be elicited by the drug, for example, morphine is more efficacious than aspirin as an analgesic
Therapeutic efficacy
The efficacy of treatment depends not only on the relative potency and efficacy of the drug but also on many pharmacokinetic and pathophysiological variables.
Therapeutic index (TI): (“pharmacodynamics”)
An index of drug safety margin and is defined as the ratio of the median lethal dose to the median effective dose. When the higher the value of the therapeutic index, the safer is a drug, e.g. penicillin has a high TI.

- LD50: Dose of a drug, which is lethal for 50% of the population
- ED50: Dose of a drug, which produces the desired effect in 50% of the population
Drugs with Narrow TI require regular drug level monitoring to ensure effective treatment without unacceptable adverse effects, for example, are Digoxin, Cyclosporine, Theophylline, Warfarin, etc.
Therapeutic window
The therapeutic window is the range of dosage of a drug that can be used effectively without unacceptable adverse effects.
- The ranges from minimum effective dose to minimum toxic dose
- Below the therapeutic window, the dose is ineffective to treat
- Above the therapeutic window, toxicity appears frequently
- Useful more than TI for clinical management purpose as a safety measure and dosage guide
Combined effects of drugs: (“pharmacodynamics”)
- Synergism
- Additive
- Supra-additive
- Antagonism
- Physical
- Chemical
- Physiological/functional
- Receptor
Synergism
When two or more drugs are administered simultaneously, their combined effect is greater than that elicited by either drug alone, for example, Sulfamethoxazole +trimethoprim; pyrimethamine +sulfadoxine.
Supra-additive (potentiation)
The enhancement of the action of one drug by other drugs. The effect of drug A+B greater than the effect of drug A+ Effect of drug B, For Example, Levodopa+carbidopa; acetylcholine+physostigmine.
Carbidopa and physostigmine inhibit the decomposition of levodopa and acetylcholine, respectively, thereby enhancing their effects.
Additive effect
The combined effect of two drugs or more drugs which is equal to the sum of their individual effect. The effect of drug A+B equals the Effect of drug A+ Effect of drug B. Example: Combination of ibuprofen and paracetamol as analgesic action.
Antagonism: (“pharmacodynamics”)
The effect of one drug is decreased or terminate in the presence of other drugs. There are the following types;
Physical antagonism
They are opposing the action of two drugs due to their physical property, for example, adsorption of alkaloids by activated charcoal for alkaloid poisoning.
Chemical antagonism
They are opposing the action of two drugs due to their chemical properties, for example, antacids are weak bases; that neutralize gastric acid and are useful for peptic ulcers.
Physiological/functional antagonism
When two drugs act on different receptors or use different mechanisms for the same physiological system and have opposite effects, such as insulin and glucagon on blood sugar, histamine, and adrenaline on bronchial muscles and BP, etc.
Receptor antagonism
Drugs bind to the same receptor as an agonist and inhibit its effects and they may be competitive or non-competitive types.
Competitive antagonism
- Equilibrium type
- Both the agonist agent and the antagonist agent bind reversibly to the same site on the receptor
- Overcome reversibly by increasing the concentration of the agonist agent
- Equilibrium type
- Non-equilibrium type
- Antagonist binds to the same site on the receptor as an agonist but binding is irreversible
- The antagonist forms a strong covalent bond with the receptor
- For example, phenoxybenzamine is an irreversible antagonist of adrenaline at the alpha receptor
- Non-equilibrium type
Non-competitive antagonism
The antagonist agent binds to a different site on the receptor and that prevents the agonist from interacting with the receptor.
In this type, the antagonistic effect cannot be overcome by increasing the concentration of the agonist, for example, diazepam, and bicuculline, etc.



