
History and distribution of Trichomonas vaginalis
Trichomonas vaginalis is first observed by Donne (1836) in vaginal secretion. The prevalence of trichomoniasis varies from 5% of patients at hospitals to 75% in sex workers.
Morphology
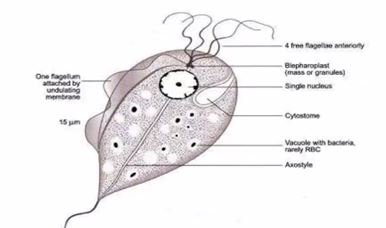
It is a pear-shaped or ovoid and size measures 10–30 μm in length and 5–10 μm in breadth with a short undulating membrane reaching up to the middle of the body.
It has anteriorly four flagella present and fifth running along the outer margin of the undulating membrane, which is supported at its base by a flexible rod, costa.
A prominent axostyle runs throughout the length of the body & projects posteriorly like a tail & the cytoplasm shows prominent or noticeable siderophillic granules, which are most numerous alongside the axostyle and costa. It is motile with a rapid jerky or twitching type of movement.
Habitat:
- In females: Vagina and cervix but may also be found in Bartholin’s glands, urethra, and urinary bladder.
- In males: Mainly in the anterior urethra, and may also be found in the prostate and preputial sac.
Life cycle of Trichomonas vaginalis
The life cycle of Trichomonas vaginalis is completed in a single host either female or male.
Mode of transmission
- Sexual transmission (It is because the trophozoite cannot survive outside and so the infection has to be transmitted directly from person to person).
- Babies may get a chance to infected during birth.
- Fomites (towels) have been implicated in transmission.
The trophozoites divide by binary fission and cysts are not formed, the trophozoite itself is the infective form. The incubation period is roughly 10 days.
Pathogenesis
The particularly infects squamous epithelium and not columnar epithelium and it secretes cysteine proteases, lactic acid, and acetic acid, which disrupt the glycogen levels and lower the pH of the vaginal fluid.
- An obligate parasite and cannot live without association or interrelation with the vaginal, urethral, or prostatic tissues.
- Trichomonas vaginalis causes petechial hemorrhage (strawberry mucosa), metaplastic changes, and desquamation of the vaginal epithelium.
- The intracellular edema present & so-known as chicken-like epithelium (the most characteristic feature of trichomoniasis).
Clinical features
The infection is often or frequently asymptomatic, but particularly in males, may develop urethritis, epididymitis, and prostatitis.
In females, severe pruritic vaginitis with an offensive, yellowish-green, often frothy discharge, dysuria, and dyspareunia may produce. Cervical erosion is most common and Endometritis and pyosalpingitis are infrequent complications.
In infants born to infected mothers, neonatal pneumonia and conjunctivitis but rarely seen.
The incubation period of trichomoniasis is ranging 4 days to 4 weeks.
Laboratory diagnosis
Microscopic examination:
- In female vaginal or urethral discharge is examined microscopically in saline wet mount preparation for characteristic jerky and twitching motility and shape. In males, in urine or prostatic secretions trophozoites may be found.
- Some fixed smear may be stained with acridine orange, Papanicolaou, and Giemsa stains.
Direct fluorescent antibody (DFA): This method of detection or identification of parasites and is more sensitive than the wet mount.
Culture:
Culture is recommended when direct microscopy is negative and it is considered as a ‘gold standard‘ as well as the most sensitive (95%) method for the diagnosis of T. vaginalis infection.
It grows best at 35°–37°C under anaerobic conditions and the optimal pH for growth is 5.5–6.0. It can be grown in various media such as solid or liquid media, tissue culture, and eggs. Cysteine-peptone-liver-maltose (CPLM) medium and plastic envelope medium (PEM) are often most commonly used.
Serology:
- ELISA Test: It is used to demonstrate or determine Trichomonas vaginalis antigen in vaginal smear using a specific monoclonal antibody for 65-KDA surface polypeptide of T. vaginalis.
Molecular method:
- DNA hybridization and PCR are highly sensitive (about 97%) and specific (about 98%) tests for the diagnosis of trichomoniasis.
- In PCR: on urine sediment rather than urethral swabs in males improves detection rates.
Other tests:
- Determination of vaginal pH method.
- Whiff or amine odor test: Positive in trichomoniasis and in bacterial vaginosis; a vaginal swab is collected and is mixed with 10% KOH for the presence of polyamines; a strong fishy odor is released due to the production of amines.
Treatment:
Simultaneous treatment is required for both partners.
- Metronidazole 2 g orally as a single dose or 500 mg orally twice a day for 7 days is the first choice of drug.
- In patients not responding to treatment with the standard regime, the dose of metronidazole may be increased or may be administered parenteral route.
- In Metronidazole resistant case Tinidazole found to be useful.
- Metronidazole is safe in the second and third trimesters of pregnancy.
- Metronidazole contraindicated in pregnancy due to its teratogenicity; topical clotrimazole by applying vaginal suppositories in a dose of 100 mg a day for 6 days.
- Abstinence from sex until the patient and their sex partners are treated.
- Testing for other sexually transmitted diseases including HIV should be performed in persons infected with T. vaginalis.
- Follow-up: It is because of the high rate of reinfection among women treated for trichomoniasis (17% within 3 months in one study), retesting for T. vaginalis is recommended or suggested for all sexually active women within three months following initial treatment.
Prophylaxis:
The prevention method is the same as for other sexually transmitted diseases.
- Avoidance of sexual contact with infected partners and the use of barrier methods (like a condom) during intercourse prevent the disease.
- The patient’s sexual partner should be tested when necessary.
- No vaccine was available.


