What is the physiology of the pain?
Pain (physiology of the pain) is defined as a stimulus that can capable of damaging or causing harm to the tissue is a nociceptive stimulus and the sensation elicited is called nociception which is pain sensation.
“Or”
Pain is an unpleasant sensory stimulus experience that leads to tissue damage. It is considered a protective mechanism and the nociceptive (pain sensitive) stimuli which are different for different tissues in the body.
Types of stimuli
- For skin: burning, Pricking, cutting, crushing, etc. that occur in the skin.
- For Gastrointestinal tract: The spasm or distension of smooth muscle in GIT, Inflammation of mucosa, and traction on the mesenteric attachment.
- In skeletal muscle: Necrosis, hemorrhage, Ischemia, injection of an irritating solution, and injury occur in the connective tissue sheath in the skeletal muscle.
- In brain: Traction on meningeal structures or cerebral arteries in the brain
- In cardiac muscle: Inflammation or ischemia to the cardiac muscle
- In joints: Inflammation of synovial membrane in the joint, exposure to hypertonic (greater concentration of solutes) saline solution, and tearing or stretching of ligaments present in the joint.
- For blood vessels: Vein or Artery pierced by the needle, inflammation, obstruction of the vessel, excessive arterial pulsation like migraine, etc.
- In nerves: Compression of a nerve root or sensory ganglia in the nerve (in intraneural lesion from the sheath of nerves.)
Types of the physiology of the pain
Pain is mainly divided into 2 types as Fast pain and slow pain. The receptors mainly Free nerve ending(non-adapting) and stimulus for pain are mechanical, thermal, chemical, etc.
Fast pain
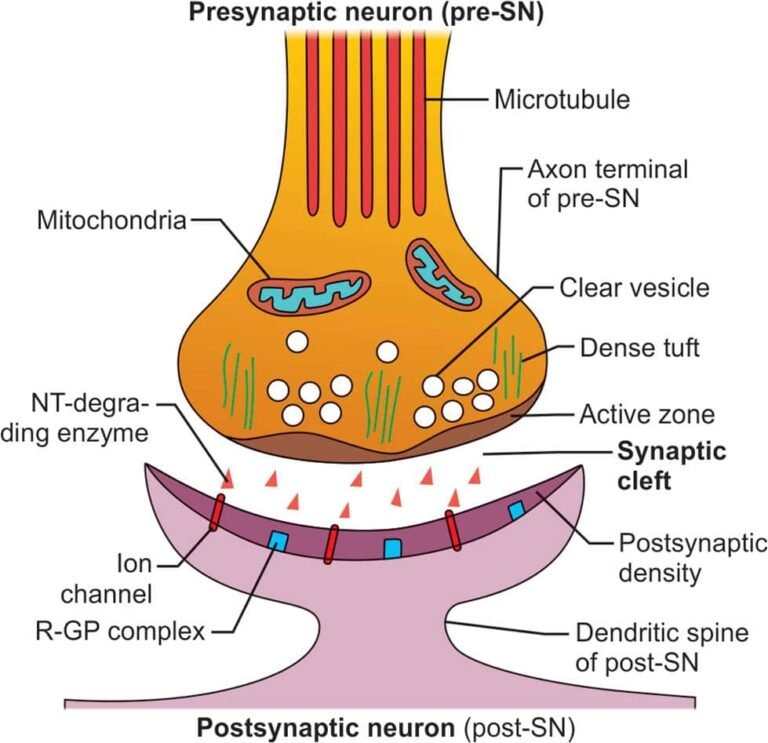
It is a sharp pain/ pricking pain/ pain from superficial structures like skin and subcutaneous tissue. The fast pain is felt within about 0.1sec after the stimulus present. The receptor is stimulated by mechanical or thermal pain stimuli. A delta fiber carries it & terminates in lamina I and V, velocity about 6-30 m/sec. The neo-spinothalamic tract is the main pathway which is Well localized in the fast pain and neurotransmitter(NT) is glutamate and neuropeptides (substance P) at the spinal cord level.
Slow pain
The slow-burning type of pain/ aching pain, throbbing pain/ pain from deep structures like bones and muscles. It is elicited by chemical types of pain stimulus( persisting mechanical or thermal).In the slow pain, type C fiber carries it & terminates in lamina II in the dorsal horn, and velocities 0.5 -2m/sec. In this pain, the paleospinothalamic tract pathway has the main role and it is poorly localized. The neurotransmitters are glutamate, substance P at the spinal cord level.
Other types of pain
- Superficial Pain vs Deep Pain: Those pain elicited in the superficial structures like skin and subcutaneous tissues is called superficial pain( fast pain). The pain is felt in the deeper structures like bones, muscles, connective tissue which is called deep pain( slow pain).
- Somatic Pain vs Visceral Pain: The pain which is originating in the somatic structures is called somatic pain and those pain originating in the visceral structures is called visceral pain.
- Peripheral Pain vs Central Pain: The pain that occurs due to direct stimulation of receptors/ nerves is known as peripheral pain( i.e.neuropathic or neurogenic pain in neuralgias). The stimulation of central pain fibers that result in pain is called central pain(i.e.pain occurs below the level of lesion in spinal transection).
Physiology of the Pain pathway
The physiology of the pain pathway helps to transmit pain to the higher centers in the brain in the lateral spinothalamic tract of the anterolateral system. They are two types of the physiology of the pain pathway such as the paleospinothalamic and neo-spinothalamic pathway.

Paleospinothalamic Pathway
It is the oldest pain pathway and mainly carries the sensation of slow pain.
The pathway is a multi-neuron slow conducting system that can mediate the poorly localized pain from deep and visceral structures. It is mainly associated with C fibers.
The order of neurons is First-order, second-order, and third-order.
- First-order neurons:
- The neurons enter into the spinal cord and terminate mainly into the lamina II of the dorsal horn of the spinal cord.
- Second-order neurons:
- Decussates and ascend up in the contralateral spinothalamic pathway and the fiber are mainly medially placed in the tract.
- In this pathway, the way to the thalamus, fibers project to 3 major nuclear groups forming three systems such as spinoreticulothalamic pathway, fibers project to the midbrain nuclei (spinomesencephalic fibers), and spinohypothalamic fibers system.
- Third Order neurons:
- In the neurons, these fibers terminate in the medial nuclear group of the thalamus from where third-order neurons arise and project on different areas of the cortex.
Features of the paleospinothalamic pain pathway
- It is mainly transmitted slow pain which is poorly localized
- Slow pain always keeps a person awake.
- The pathway evokes the emotional experience of pain and mediates autonomic responses.
Neospinothalamic pain pathway
The pain pathway is mostly developed in primates and it carries fast pain mainly. It is associated with mostly Aδ fibers and the order of neurons are first-order neurons, second-order neurons, third-order neurons.
- First Order Neurons: The mostly first-order neurons are terminate principally in the lamina I and V in the dorsal horn of the spinal cord and the neurotransmitters are released at the terminals of primary nociceptive afferents such as glutamate and neuropeptides (substance P).
- Second-order neurons: The neurons cross to the opposite side in the same segment of the spinal cord and ascend in the lateral spinothalamic tract. In the spinal cord, there is a various topographic organization with a lot of fibers.
- Third-order neurons: The neurons originate from specific nuclei of the thalamus and project into the postcentral gyrus in the sensory cortex in the brain.
Features of the neo-spinothalamic pain pathway
- There is a topographic organization of fibers present in the thalamus and cortex that is very concrete, and in the sensory cortex, and most of the neurons are organized in modality-specific columns. Therefore, the fast pain is better localized in this pathway.
- The termination in the specific and discrete areas in the thalamus and cortex, sub-serves the sensory-discriminative aspects of pain which is the localization of pain and detection of quality and intensity of the noxious stimuli in the pathway.
The endogenous pain relief system
It is also known as the central analgesia system when inbuilt for pain reduction. It consists of three components which are the following
- The periaqueductal gray & periventricular area
- The raphe Magnus nucleus
- Pain inhibitory complex situated in the dorsal horn of the spinal cord
Gate control theory of pain
According to this, pain can be modulated systemically by the peripheral mechanisms, especially by gating the impulses in the spinal cord.
The collaterals from large myelinated afferent fibers associated with tactile sensation produce presynaptic inhibition in the dorsal horn of the spinal cord.
Thus activity in large afferent fibers regulate (act as a gate) and maintain transmission of impulses originating in pain receptors. For example, acupuncture and balm.
Referred pain (physiology of the pain)
The pain perceived in somatic structure due to visceral irritation or injury is known as referred pain.
The visceral pain is not referred to the skin which overlying the viscera but to the other areas of the skin which is innervated by the same embryonic spinal segment,
For example, in acute myocardial infarction (AMI), the pain is referred into the left arm of the inner aspects, acute cholecystitis pain is referred to the right shoulder.
Theory of referred pain
The referred pain can be explained by the following theory,
- Dermatomal theory
- Convergence theory
- Facilitation theory
- Experience theory
Dermatomal theory
When visceral pain is referred to, it usually refers to those structures that can develop from the same embryonic segment. For example, the heart and the inner aspect of the arm develop from the same embryonic segment so, the pain of acute myocardial infarction radiates to the ulnar border of the left arm.
Convergence theory
When the visceral and the somatic afferent fibers converge on the second-order of neuron in the spinothalamic tract pathway i.e. the fibers carrying the pain sensation from the somatic structures also carry the pain from the visceral structures. The cortex sometimes can’t differentiate the site of origin so the signal conveyed by the brain for perception is also referred to as the somatic area in addition to the projection to the viscera.
Facilitation theory
In this theory, the collaterals arising from the visceral afferent fibers project to the spinothalamic neurons that receive afferents from somatic structures. So, the pain sensation arising from a somatic structure is facilitated (strengthened) by the activity in the visceral afferent. Thus, minor activity in some somatic afferents can cause pain.
Experience theory
This theory has a role in the genesis of referred pain. When the pain instead of being felt at its usual site, it may be referred to some other structure or area in which the patient had experienced pain earlier. For example, pain due to the inflammation of the abdomen viscera is usually referred to as the site of the midline. But, in the patients with a previous history of surgery of the abdomen, the pain is referred to as a surgical scar, which may not be in the midline
Clinical abnormalities of pain (physiology of the pain)
- Hyperalgesia: When the increased sensitivity and lowered threshold to painful stimuli. Inflammation of the skin is the main cause.
- Hypoalgesia/ Hypalgesia: When the decreased sensitivity and raised threshold to painful stimuli.
- Analgesia: The complete loss of pain sensation. It may not be associated with the loss of other sensations.
- Hyperpathia: In this condition, the defect in pain perception i.e.associated with an increased reaction to the pain stimulus once it is perceived. Or, it is the exaggerated response to pain stimuli. In this condition, there is also an increased reaction to other types of stimuli.
- Allodynia: This is a state in which there is an excessive response to the various types of mild stimuli. For example, some stimulus like light touch which is never painful elicits pain in allodynia.
- Herpes Zoster infection: It is a type of neuropathic pain in which the injury to the nerves results in this type of pain. The Herpes Virus infects a dorsal root ganglion, and which causes pain in the dermatomal segment served by the ganglion.
- Tic douloureux: It is also known as trigeminal neuralgia. In these abnormalities of the pain, the lancinating pain occurs in some people on the sensory distribution area of the V or IX cranial nerve.
- Causalgia: It is a burning pain that usually develops following a traumatic peripheral nerve injury.
- Inflammatory Pain
- Neuropathic Pain