
What is lead poisoning?
Lead poisoning is a serious health concern that occurs when an individual accumulates high levels of lead in their body. Lead is a toxic heavy metal that can have detrimental effects on various organ systems, particularly the nervous system, kidneys, and blood cells.
What are the sources?
Lead poisoning occurs through exposure to lead-containing substances. These are most common sources of lead exposure that include;
- Lead-based paints
- Contaminated soil, dust, drinking water from lead pipes or plumbing fixtures
- Certain types of pottery or ceramics, imported cosmetics, and certain traditional remedies or cosmetics.
Children are particularly vulnerable to lead poisoning due to their hand-to-mouth behaviour and the fact that their growing bodies absorb lead more easily than adults.
Occupational exposure to lead is also a concern for adults working in the construction, battery manufacturing, and painting industries.
Toxic compounds and uses
Compounds | Uses |
Lead acetate (sugar of lead) | Earlier used as an astringent and local sedative for sprains |
Lead tetraoxide (red lead or vermilion) | Used as sindoor |
Tetraethyl lead | Antiknock for petrol |
Lead sulfide (surma; least toxic) | Applied on the eyes |
Lead carbonate (white lead) | Manufacture of paints |
Mode of Action
When lead enters the body, it can be absorbed into the bloodstream and distributed to various organs and tissues. The primary mechanism of lead toxicity involves its interference with the functioning of enzymes and proteins involved in crucial biological processes.
Lead displaces essential metals such as calcium, zinc, and iron, disrupting their normal roles in enzymatic reactions and cellular processes. This interference can lead to oxidative stress, mitochondrial dysfunction, and disruption of neurotransmitter signalling, resulting in cellular damage and dysfunction.
or,
It is combined with sulfhydryl groups; a certain substance can interfere with various processes in the body, including mitochondrial oxidative phosphorylation, ATPases, and calcium-dependent messengers. Furthermore, it disrupts the action of enzymes that are vital for heme synthesis.
This leads to the enhancement of oxidation and cell apoptosis, ultimately resulting in hemolysis. Additionally, the substance has deleterious effects on nerve cells and the myelin sheath, causing cerebral oedema.
Clinical Features (Acute poisoning)
Gastrointestinal Clinical features
- Metallic taste
- Dry throat, thirst
- Nausea, vomiting
- Colic abdomen pain
- Blood stained diarrhoea
- Peripheral circulatory collapse
CNS clinical features
- Headache
- Lethargy
- Arthralgia
- Myalgia
- Anorexia
- Insomnia
- Paresthesia
- Depression
- Coma, death
Postmortem findings (Acute Lead Poisoning)
- Body appears emaciated
- Rigor mortis appears early
- Stomach wall is swollen, mucous membrane is congested, grayish in color and softened with eroded patches
Chronic Lead Poisoning (Plumbism/Saturnism/colica pictorum (painter’s colic)/ Devonshire colic)
Lead is a dangerous substance that acts as a cumulative poison in the human body. When lead is ingested or inhaled, it tends to accumulate in the bones in the form of phosphate and carbonate compounds. However, certain circumstances can lead to the release of lead from the bones into the bloodstream.
One such situation is a calcium deficiency, where the body tries to compensate by mobilising calcium from the bones, inadvertently releasing lead along with it.
Additionally, other factors such as acidosis (excessive acidity in the blood), fever, sweating, consumption of alcohol, and exposure to sunlight can also promote the release of lead from the bones.
It is worth noting that the daily intake of lead should be strictly limited, with the recommended amount being 1-2 milligrams to avoid the harmful effects of lead poisoning.
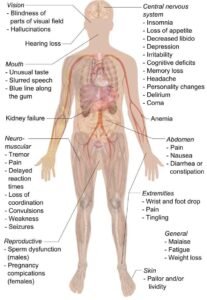
Clinical Features (Chronic Lead poisoning)/ Plumbism clinical features
Mnemonic:@ABCDEFGHI
- A-Anemia, Anorexia, Arthralgia, Abortion, Atrophy of optic nerve
- B-Basophilic staining, Burton’s line
- C-Constipation, Colic, Coproporphyrin excess in urine, Cerebral edema
- D – Drop (wrist, foot)
- E – Encephalopathy/ Emaciation
- F – Facial pallor, Foul-smelling breath, Failure of Kidneys, Fanconi syndrome
- G – Gonadal dysfunction/ Saturnine Gout
- H – Hypertension/ Headache/ Hallucination/Hyperesthesia
- I – Impotence/ Infertility/ Insomnia/ Irritability
Postmortem Findings (Chronic lead poisoning)
- Blue line seen in gums
- Paralysed muscle show fatty degeneration
- Heart may be hypertrophied, atherosclerosis of aorta
- In intestine, ulcerative/hemorrhagic changes with contraction and thickening
- Liver and kidney get contracted and hard
- Brain is pale and swollen
- On histology- bone marrow shows hyperplasia of leucoblast and erythroblast
Diagnosis
- History and Clinical features
- Lab tests
- Whole Blood lead level >70 μg/dl (severe toxicity) and >50–70 μg/dl (moderate toxicity)
- Coproporphyrin in urine >15 μg/dl
- δ-amino levulinic acid in urine >5 mg/l
- Normocytic, normochromic or a microcytic, hypochromic anemia may be seen with mixed etiology
- Punctate basophilia: > 200 cells/cu mm
- Elevated free erythrocyte protoporphyrin or zinc protoporphyrin (>35 μg/dl) level and azotemia
- Urine lead level > 80 μg/dl (in 24 hours sample)
Treatment
- Remove the patient from source of exposure
- Potassium or sodium iodide 1-2 gram 3 times a day orally
- Sodium bicarbonate 20–30 gram in four or five divided doses orally
- Saline purgatives like MgSO4 or sodium sulfate 8–12 g orally
- Calcium disodium versanate as deleading agent
- Dietary supplement (Fe, Ca, Mg, Zn)
- Chelating therapy
- For adults (severe toxicity) and children with encephalopathy: CaNa2EDTA
- For mild to moderate toxicity: DMSA (succimer)
- For renal impairment: BAL
- Mannitol for cerebral edema, and diazepam IV for seizures associated with lead encephalopathy
- Hemodilaysis in cases of renal failure
- Symptomatic treatment
Medico-legal aspects
- Acute and homicidal poisoning is rare
- Chronic poisoning is more common and regarded as industrial disease
- Not used for suicide
- Accidental chronic poisoning occurs in people working with lead
- Red lead is used locally for abortion
- Also used alone or mixed with arsenic as cattle poison.
- A person can developed lead poisoning from retained lead bullet in the tissue in 12 to 48 days
References
- Gautam Biswas, Review of forensic medicine and toxicology, 4th Edition
- Nagesh kumar G Rao, Textbook of Forensic Medicine and Toxicology, 2nd Edition
- Dr KS Narayan Reddy, The essentials of forensic medicine and toxicology, 33rd Edition
- Krishnan Vij, Textbook of Forensic Medicine and Toxicology, 5th Edition
- Casarett and Doull’s – Essentials of Toxicology
