Overview
The Wilms tumor (Nephroblastoma) is the most frequent primary tumor of the kidney in children. It is a highly malignant primary embryonal tumor.
- Age group: Most common between 2-5 years of age children and more than 95% occurs below 10 years of age.
Pathogenesis of Wilms Tumor (Nephroblastoma)
- In most (90%) cases, the Wilms tumor (Nephroblastoma) is sporadic and unilateral.
- About 5-10 % are bilateral and involves either simultaneously (synchronous) or one after another (metachronous).
- Mutation in tumor suppressor genes is associated with Wilms tumor (Nephroblastoma) and these include Wilms tumor-associated genes 1 (WT1) and WT2.
- WT1 gene is located on chromosome 11p13.
- In about 5% of cases, Wilms tumors emerge in three congenital syndromes at an early age and often bilaterally.
Wilms’ Tumor (Nephroblastoma) Associated congenital syndromes are:
- WAGR syndrome
- Denys-Drash syndrome
- Beckwith-Wiedmann syndrome.
WAGR (for Wilms tumor, aniridia, genital anomalies in the body, and mental retardation) syndrome:
- It has germline deletions of 11p13, a region where Wilms tumor-associated gene (WT1) is located.
Denys-Drash syndrome(Wilms tumor, intersexual disorders, glomerulopathy) :
- It is associated or related to mutations of the WT1 gene.
Beckwith-Wiedemann syndrome (BWS):
- It is associated or related to Wilms tumor and WT2 gene imprinting abnormalities.
-
- Mutations of the β-catenin gene & are found in some sporadic cases of Wilms tumors.
- Nephrogenic rests (small foci of persistent primitive blastemal cells, which are precursor lesions of Wilms tumors) are seen in the renal parenchyma adjacent to bilateral Wilms tumors(Nephroblastoma).
- Wilms tumor was also found in association with other different malignancies conditions such as (e.g. osteosarcoma, retinoblastoma, hepatocellular carcinoma, and neuroblastoma).
Morphology of Wilms Tumor (Nephroblastoma)
Gross

- Usually large, single, round, well-circumscribed mass.
- It generally unilateral but 10% is either bilateral or multicentric.
Cut section
- The tumor is soft, bulging, homogeneous, and tan to gray.
- Cyst formation, Foci of hemorrhage, and necrosis may be seen.
Microscopy
Three components such as,
- Blastemal
- Immature stromal
- Immature epithelial
- These three major components of tumors, which resemble normal fetal tissue, and these cells attempt to recapitulate different stages of nephrogenesis.
- The three types of cells are:
Blastemal component:
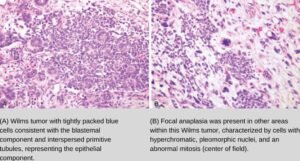
- It consists of small, round to oval blue cells with the presence of minimal cytoplasm and arranged in sheets, nests, and trabeculae.
Immature stromal (mesenchymal) component:
- This component consists of undifferentiated fibroblast-like spindle cells.
- It may show skeletal muscle, smooth muscle, or fibroblast differentiation.
Immature epithelial component:
- These epithelial cells show differentiation in the form of small abortive (embryonic) tubules of immature glomeruli.
- Classically, the tumor shows a triphasic phase of all three types of cells combination, although the percentage of each component varies.
- Occasionally biphasic (contain only two elements) or monophasic (even only one).
Anaplasia: Anaplasia can be defined as the presence of cells with large, hyperchromatic, pleomorphic nuclei, and atypical mitotic figures. It is associated or related to TP53 mutations and such tumors do not respond to chemotherapy.
Clinical Features
- Abdominal mass
- Microscopic hematuria
- Occasionally, intestinal obstruction is a result of pressure from the tumor.
Spread through:
- Local spread: It spreads to perirenal soft tissues.
- Lymphatics: It spreads to regional lymph nodes.
- Hematogenous: Lungs, liver, and peritoneum.
Prognosis of Wilms tumor
Clinical parameter
- Children younger than 2 years of age have a better chance of prognosis.
Histological parameter
- The invasion of the renal capsule is associated with a poor prognosis.
- Anaplasia indicates a poorer prognosis.