Introduction to Hyaline Membrane Disease (HMD)
Definition
Hyaline membrane disease, also known as respiratory distress syndrome in newborns, is a common problem in preterm infants (<34 weeks). It is defined as difficulty in respiration starting shortly after birth due to primarily deficiency of pulmonary surfactant in the lungs.
Risk factors and Etiopathogenesis
Risk Factors
There are the following risk factors associated with Hyaline membrane disease/RDS
- Prematurity and low birth weight
- Cesarean section without labor
- Infant of diabetic mother
- Hypothermia
- Early cord clamping (<1 minute)
- Chorioamnionitis
- Precipitous delivery (extremely fast labor and delivery)
- Others e.g. boys>girls, genetic conditions, second twin
Etiopathogenesis of Hyaline Membrane Disease
- Respiratory distress syndrome (RDS) is caused by pulmonary surfactant deficiency.
- Surfactant is a lipoprotein containing phospholipids and proteins.
- It is produced by type II alveolar cells (type II pneumocytes) and reduces surface tension in the alveoli.
- Without surfactant, surface tension increases, leading to alveolar collapse during expiration.
- More negative pressure is needed during inspiration to keep the alveoli open.
- This leads to inadequate oxygenation and increased work of breathing.
- Hypoxemia and acidosis result, causing pulmonary vasoconstriction and right-to-left shunting across the foramen ovale.
- This worsens hypoxemia, eventually leading to respiratory failure.
- Ischemic damage to the alveoli causes the transudation of proteins, forming a hyaline membrane.
- Surfactant production starts around 20 weeks of life and peaks at 35 weeks gestation.
- Therefore, neonates less than 35 weeks are prone to developing RDS.
Clinical Features of Hyaline Membrane Disease
Signs and Symptoms
The symptoms of RDS occur within the first six hours of birth in a preterm baby, as shown by
- Respiratory distress
- Fast breathing (>60 breaths/min)
- Retraction of intercostal and subcostal space
- Nasal flaring
- Chest indrawing
- Grunting (partial closure of the glottis during the forceful expiration to maintain functional residual capacity)
- Cyanosis (bluish discolouration of the skin) in room air
- Falling Oxygen saturation (SpO2<90%)
- Hypotension (Decreased blood pressure)
- Decreased air entry on auscultation
Diagnosis of Hyaline Membrane Disease
The diagnosis of HMD in newborns is based on clinical features and some support from investigations. There are the following investigations and their findings:
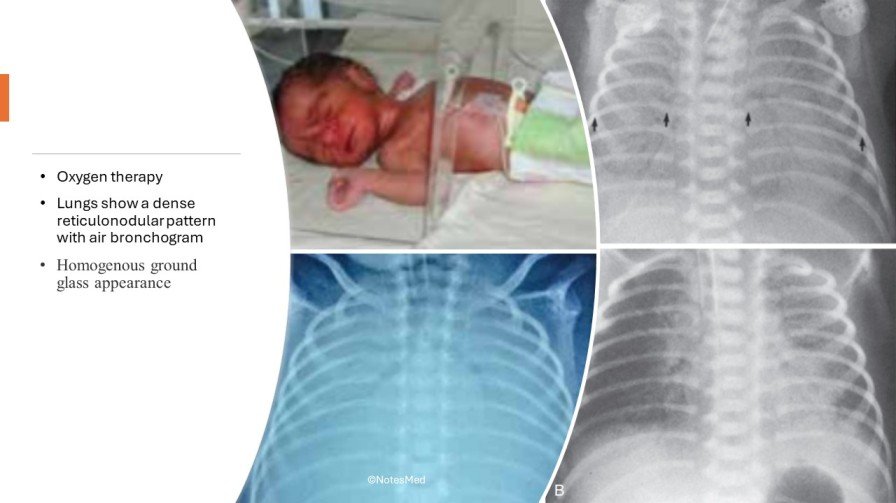
- Chest X-ray: Homogenous ground glass appearance, a complete white out of lungs (loss of demarcation of heart borders) in severe disease, air bronchogram, reticulogranular pattern, Low lung volume, air leaks (e.g. pneumomediastinum and pneumothorax)

- Lecithin/Sphingomyelin ratio: 2:1 denotes fetal maturity
- Shake test of gastric aspiration (Helps to determine lung maturity)
- Blood (Sepsis screen)
- Complete blood count (CBC), Peripheral blood Film: non-specific
- C-reactive protein (CRP), procalcitonin: raised (if infection)
- Blood culture
- ABG (arterial blood gas): Low O2, high CO2, low pH
- Serum electrolyte: Dyseletrolytaemia

Management of Hyaline Membrane Disease
Supportive management
- Keep the baby warm e.g. Baby covered with warm clothes, Keeping under radiant warmer.
- Nil per oral and appropriate IV fluids (10 % dextrose
- Respiratory support: Clearing the airway, giving O2 through the headbox, until the lungs start producing enough surfactant. If a baby does not improve and develops difficulty in breathing with falling SpO2, then keep the baby on continuous positive airway pressure (CPAP)
- Regular bedside monitoring of respiratory status (cyanosis, respiratory rate, rhythm and pattern, SpO2, air entry), circulatory status (Capillary refill time, Heart rate, Blood pressure), body temperature, capillary glucose status
- ABG analysis
- If sepsis, IV antibiotics (Ampicillin + gentamicin)
Specific Management of Hyaline Membrane Disease
- Maintain oxygenation and surfactant therapy
- InSurE: Intubation-surfactants- extubate rapidly to CPAP
- Extracorporeal membrane oxygenation (ECMO) may be done in some cases.
- Use of surfactant through Endotracheal tube
- Apnea management: physical stimulation, aminophylline, caffeine, mechanical ventilation
Complications Respiratory Distress Syndrome
There are the following common complications listed:
- Pulmonary complications: collapse, pulmonary haemorrhage, pneumothorax, Bronchopulmonary Dysplasia (BPD)
- CNS complications: Intraventricular haemorrhage, Retinopathy of prematurity
- Cardiac complications: Patent ductus arteriosus (PDA)
- GIT complications: Necrotizing enterocolitis
- Renal: Acute Kidney Injury
- Septicemia
Prevention of Respiratory Distress Syndrome
- Antenatal glucocorticoids to mother <34 weeks of gestation:
- Injection of Betamethasone 12 mg doses, IM 24 hours apart (2 doses)
- Injection of Dexamethasone 6 mg doses, IM 12 hourly for 2 days (4 doses)
- Prophylactic surfactants via ET tube in gestation <28 weeks or weight<1000 gram
- Basic neonatal care
Prognosis
Infants managed with antenatal steroids, respiratory support, and surfactant therapy have an excellent prognosis, with mortality less than 10%. Survival rates can reach up to 98% with advanced care. However, in low-income countries without intervention, mortality rates for premature infants with RDS can be close to 100%. With ventilatory support, surfactant production begins, and RDS improves within 4 or 5 days. Untreated disease can lead to severe hypoxemia, multiple organ failure, and death.
Conclusions of Hyaline Membrane Disease
- Hyaline membrane disease (HMD) is a common problem in preterm infants (<34 weeks), characterized by respiratory distress due to surfactant deficiency.
- Risk factors include prematurity, low birth weight, caesarean section without labour, infant of a diabetic mother, hypothermia, early cord clamping, chorioamnionitis, and precipitous delivery.
- Respiratory distress syndrome (RDS) is caused by surfactant deficiency, leading to increased surface tension, alveolar collapse, and inadequate oxygenation.
- Symptoms include fast breathing, chest indrawing, nasal flaring, cyanosis, and decreased oxygen saturation.
- Diagnosis is based on clinical features and investigations such as chest X-ray and blood tests.
- Treatment includes supportive measures like warmth, IV fluids, and respiratory support, along with specific treatments like surfactant therapy and ECMO.
- Complications include pulmonary, CNS, cardiac, GIT, renal issues, and septicemia.
- Prevention strategies include antenatal glucocorticoids, prophylactic surfactants, and basic neonatal care.
- Prognosis is excellent with proper management, but mortality rates are high without intervention, especially in low-income countries.
Differential diagnosis
- Transient tachypnea of the newborn
- Pulmonary air leak disorders (pneumothorax, pneumomediastinum)
- Neonatal pneumonia
- Meconium aspiration
- Persistent pulmonary hypertension of the newborn
Commonly Asked Questions
Three major signs of respiratory distress:
- Fast breathing (>60 breaths/min)
- Retraction of intercostal and subcostal space
- Nasal flaring
There are four most common causes of respiratory distress:
- Prematurity and low birth weight
- Caesarean section without labour
- Infant of diabetic mother
- Hypothermia
How to treat respiratory distress syndrome in children:
- Supportive management (e.g., keeping the baby warm, respiratory support)
- Specific management (e.g., maintaining oxygenation, surfactant therapy)
- Monitoring respiratory and circulatory status
- Treatment of complications
Acute Respiratory Distress Syndrome (ARDS) is typically classified into three categories based on its onset and duration:
- Mild ARDS: This type is characterized by a ratio of arterial oxygen partial pressure (PaO2) to fractional inspired oxygen (FiO2) between 200 and 300 mm Hg with PEEP or CPAP of at least 5 cm H2O. These patients have mild to moderate respiratory distress.
- Moderate ARDS: This type is characterized by a PaO2/FiO2 ratio between 100- and 200-mm Hg with PEEP of at least 5 cm H2O. These patients have significant respiratory distress.
- Severe ARDS: This type is characterized by a PaO2/FiO2 ratio of less than 100 mm Hg with PEEP of at least 5 cm H2O. These patients have severe respiratory distress and are at high risk of mortality.
Powered By EmbedPress