Overview of Measles
What is measles?
Measles is a highly infectious (contagious) disease at the community level and characterized by fever, malaise, cough, coryza (rhinitis), and conjunctivitis followed by a generalized maculopapular rash. It is also called rubeola, red measles, hard measles, and 7-day measles. Measles virus causes measles and which is a single-stranded negative-sense RNA virus of the genus Morbillivirus and the family belongs to Paramyxoviridae.

Epidemiology
Human beings are the only reservoir for this virus; unvaccinated infants who have lost their maternal antibodies account for a large proportion of susceptible individuals.
It is generally most common in childhood, However, as vaccine coverage increases, the age of distribution of the disease shifts upward. In the United States, adolescents and adults are the most probable age groups to acquire measles.
Between 2000 and 2016, the yearly incidence of measles decreased by around 87%. Only one WHO region (Americas) has been verified as having eliminated measles.
Since the elimination of measles in 2000 in the United States, outbreaks in the United States occurred predominantly among knowingly unvaccinated children (in between 59 – 93%).
As of October 2017, 120 new cases of measles reported to CDC from 15 states, striking the number of cases reported in 2016; 65 new confirmed cases were identified in a Somali-American community from Minnesota due to a decrease in MMR vaccination coverage.
Measles has not been endemic in the United state; however, a limited number of cases occur annually due to importations of viruses from endemic countries that contribute to outbreaks.
Despite sporadic outbreaks, the elimination of measles in the United States appears to have been sustained as of 2011 but increasing rates of deliberate under vaccination undermine measles elimination programs.
Infective material: Respiratory secretions of measles cases.
Period of communicability: four days before and five days after the appearance of rashes. It is highly infectious during this time period.
Secondary attack rate: About more than 90 percent.
Mode of transmission: Direct contact with large respiratory droplet infection and droplet nuclei, but the airborne spread is also possible. It is also transmitted by conjunctival route but is a controversial statement.
Risk factors:
Age: Incidence high in children (between 6 months and 3 years) in the case of developing countries. In the developed countries, there is a shift in the age of incidence due to the fact that of high immunization coverage.
Immunity: One attack of measles confers lifelong immunity and second attacks are rare. Immunity after vaccination is quite solid and long-lasting.
Nutritional status: Malnutrition increases risk. Measles becomes more severe in the case of malnourished children and the mortality is around 400 times higher than in healthy children. It is due to poor cell-mediated immunity due to malnutrition. Measles precipitates even children into malnutrition.
Sex: Equal in both the sexes.
Environmental factors: It is more common during winter and early spring (Jan to April) due to overcrowding indoors. Poor housing, overcrowding favor disease transmission.
Pathogenesis
When the virus entered your body through the respiratory tract by droplet infection, and then viruses quickly pass to the nearest lymph node, multiply there.
And leak into the bloodstream in small amounts to reach the reticuloendothelial tissues such as the spleen, liver, bone marrow, where they are multiply and destroy those cells
Then flow again into the bloodstream in your body affects the different tissues such as respiratory mucosa, alimentary mucosa, skin, and conjunctiva. The symptoms appear due to inflammatory reactions in your body.
Incubation period
It is 10 days between the onset of infection and onset of the fever and 14 days between the infection and the appearance of rashes in your body. The incubation period is 10 to 14 days.
Clinical features (sign and symptoms) of Measles
The clinical features occur in two stages such as a prodromal and exanthematous stage.
Prodromal stage (early stage):
It is also called pre-eruptive or a catarrhal stage and lasts for about 3 days and characterized by;
-
- Fever
- Anorexia
- Cough
- Conjunctival congestion
- Photophobia
- Swelling of lower lids
- Runny nose
- Flushing of the face
- Lacrimation
- Irritation, nausea, and vomiting
- Cervical lymphadenopathy
- Febrile convulsions.
- Koplik’s spots:
It is small, irregular, and red white spots on a red base, smaller than the head of the pin, looking like grains of salt on the red background with innumerable numbers present center on the mucous membrane.
The Koplik’s spots are pathognomonic of measles and appear about one or two days before the appearance of rashes.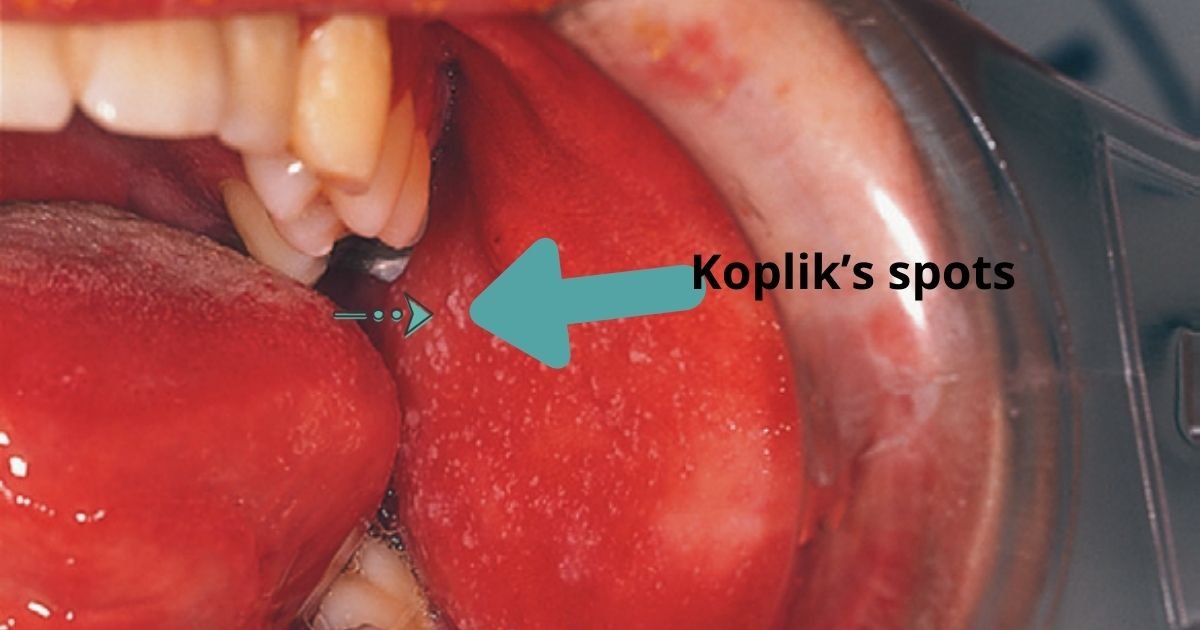

Exanthematous stage (Eruptive stage):
When rashes appear on the 4th day of fever, 1st behind the ears, then on the forehead, face, and down the trunk slowly taking 2 to 3 days to progress to the hands and lower extremities.
Rashes are pink (or dull red), maculopapular, and velvety. Rashes remain discrete but often become confluent 7 blotchy. The temperature will be very high, about 104°F.
From the 5th or 6th day, rashes start to disappear in the same order they had appeared. Lesions present in the face completely, but on the trunk, they leave behind brownish discoloration that may persist for about 5 to 8 weeks. No permanent pockmarks are left behind the lesion area.

Complications
If measles present in your body then go to the doctors and consult it. Otherwise, there are various complications that occur in your body, there are the following;
-
- Croup
- Pneumonia (bronchopneumonia): secondary infection
- Otitis media: It occurs due to secondary infection.
- Acute gastroenteritis
- Severe dehydration
- Malnutrition
- Febrile convulsions (due to very high temperature in your body)
- Multiple sclerosis
- Retrobulbar neuritis
- Toxic encephalopathy
- Conjunctivitis
- Corneal ulceration
- Encephalitis (1 out of 1000 and mortality is about 40 %)
- Subacute sclerosing panencephalitis (SSPE):
It is a very rare complication, which developed many years after the initial measles infection. In this case, the virus is trapped in the brain and exists as a latent infection.
Which is reactivated after about seven years resulting in progressive mental deterioration leading to blindness, paralysis, decerebrate rigidity, and ultimately death.
Diagnosis of Measles
Generally, Your doctor can be diagnosed with the help of characteristic features of measles such as rashes and pathognomonic Koplik’s spots.
Serologic testing:
Your doctor can be done a serological test in the lab and help to diagnose a disease, There are the following tests that will be done;
ELISA: This test used for the detection of IgM measles antibodies in your body. Measles-specific IgM is generally detectable within 1–3 days of rash onset.
Viral culture and Real-time reverse transcriptase-PCR (RT-PCR): These tests are used occasionally to detect measles. These tests are available from the CDC and some public health laboratories can help establish a diagnosis promptly.
Treatment and Management with Nursing Care
-
- Isolation in a well-ventilated room.
- Vitamin-A (for children ≥12 months: 200,000 IU daily for two days) and WHO recommended for all children with measles.
- Maintain TPR (Temperature, pressure, and respiration) chart every 4th hourly.
- Concurrent disinfection of nasal and throat secretions.
- A tepid sponge bath is given to relieve irritation of the skin and to reduce your body temperature.
- Light and clean clothes.
- Antipyretics to control fever.
- Washed your child’s eye with sterile normal saline.
- Prophylactic antibiotics used in some patients
- Attendants use gowns and masks.
- Plenty of water and fruit juice because of loss of appetite.
- Terminal disinfection of the room.
- Watch for the complications.
Prevention and control
In the United State, children are routinely immunized with two doses of a live attenuated vaccine that contains measles, mumps, and rubella (MMR) antigens.
Measles Vaccine-induced immunity lasts for at least several decades; rates of secondary vaccine failure 10–15 years after immunization are nearly 5 percent.
In contrast, a natural infection leads to life-long immunity. Measles vaccine 0.5 ml was given subcutaneously in the upper arm or anterolateral surface of the thigh.
Administration of immunoglobulin intramuscularly within 6 days of exposure, which can prevent or modify the disease in immunocompetent persons.
It is recommended in children below 1-year-old, immunocompromised patients, and pregnant women. In healthy patients 0.25 ml/kg, for immunocompromised host 0.5 ml/kg given and the maximal dose is 15 ml.