

Overview
Acute post-streptococcal glomerulonephritis is developed after streptococcal bacterial infection in children and young adults. It is the most common disorder in developing countries in the world.
Age group: Most frequently present in children between 6-10 years of age, but may develop in adults.
Etiology and Pathogenesis of Acute post-streptococcal glomerulonephritis
- Follows streptococcal infection (hence post-streptococcal infection) rather than direct primary infection of the kidney by bacteria streptococci.
- Primary streptococcal infection generally involves the part of the pharynx (pharyngitis) or the skin area (impetigo/pyoderma).
- Infections of Skin are usually associated with scarlet fever, overcrowding, and poor hygiene.
- Certain strains of group Aβ -hemolytic streptococci are nephritogenic. More than 90% are due to types 12, 4, and 1.
- The streptococcal antigenic component responsible for immune reaction in acute post-streptococcal glomerulonephritis is streptococcal pyogenic exotoxin B (SpeB) in most but not all cases.
- The latent period of 1 to 4 weeks following primary streptococcal infection.
- Immune-complex mediated disease.
Mechanism of Damage
- Immune complexes are formed in the circulation and get deposited within glomeruli.
- Immune complexes initiate inflammation via. activating complement & other humoral & cellular mediators of inflammation.
- The inflammatory mediators attract and activate neutrophils and monocytes and stimulate the proliferation of the mesangial and endothelial cells.
- The result is Hypercellular glomerulus.
Presentation (LAB FINDINGS)
- Hematuria 1-3 weeks following group A streptococcal infection.
- Periorbital edema.
Morphology of Acute post-streptococcal glomerulonephritis
Gross
- The kidneys are enlarged and show a pale capsular surface and cortex.
Microscopy
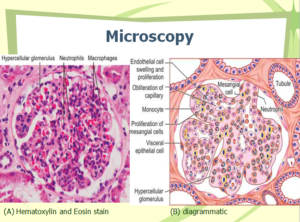
Light Microscopy (LM)
- Glomeruli:
- Increased cellularity (Proliferation of mesangial, endothelial, and neutrophils).
- The hypercellularity is due to;
- Infiltration by leukocytes (neutrophils and monocytes).
- Proliferation and swelling of endothelial and mesangial cells.
- Rarely proliferation of parietal cells lining Bowman’s capsule.
- Diffuse involvement.
- Obliteration or eradication of glomerular capillary lumen: Due to swelling and proliferation of endothelial cells & mesangial cells + infiltration by leukocytes.
- Tubules:
- Contains red cell casts in the lumen and the tubular epithelial cells may show degenerative changes.
- Interstitium:
- Edema and inflammatory cell infiltrate.
- Blood vessels: Unremarkable.
Immunofluorescence Microscopy
- Granular deposits of IgG, IgM, and C3 in the mesangium and along with the GBM →granular fluorescence.
Electron microscopy
- Sub-epithelial“humps” (Immune complexes deposit).
- Sub-epithelial deposits of discrete, amorphous, electron-dense deposits are a characteristic feature.
Clinical Course
Acute proliferative glomerulonephritis:
- Periorbital edema.
- Mild to moderate hypertension.
- An affected child develops
- Malaise
- Fever
- Nausea
- Oliguria
- Hematuria (smoky or cola-colored urine) 1 to 2 weeks after sore throat recovery.
[embeddoc url=”https://notesmed.com/wp-content/uploads/2020/08/Acute-post-streptococcal-glomerulonephritis.pdf” download=”all”]
